
What are surgical site infections?
As the name suggests, it is an infection occurring at the site of surgery. Although it commonly suggests infection at the site of skin incision or surgical wound closure, this may involve the entire field of surgery and most importantly it may have its focus well away from skin, which may be just secondarily involved. This is akin to a tumor with invisible geometry and concealed extensions.
How do we identify surgical site infection?
This is easier said than done. Classic teaching does tell us to rely on pain, redness ( erythema), altered lab parameters, imaging and even vital signs, but most importantly on needs a strong index of suspicion. Why I say this is because all of the above symptoms and signs almost always lie in a GREY ZONE and it can difficult to differentiate between usual and unusual. Often when the skin wounds starts discharging or gets dehisced, it is the showdown of the body rather than an early clinical finding.
What do we do next?
As with everything in medicine, IT DEPENDS!. While body does take care of subclinical infections via its own robust mechanisms, we do need to help the cause with antibiotics, clean dressings and optimizing all wound healing nutritional parameters. This approach is a not a blind fall-back as experiences and science has taught us that closed, moist and clean wound heal better and quicker.
But when the situation is past that point, we need to be PROACTIVE, as a failing natural healing effort, could cause profound surgical comorbidity which can be life or limb threatening and lead to permanent contractures disability over and above the anguish of loss of employment and quality life.
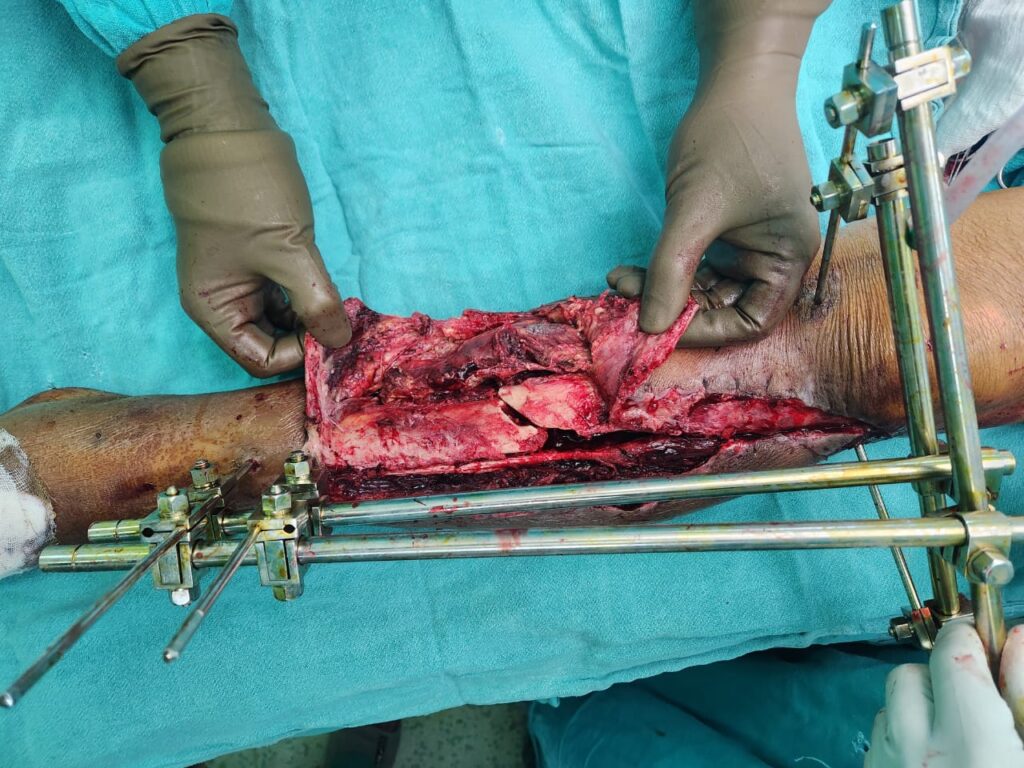
The first thing to do is debridement, which simply means taking away all the debri ( dead or de-vitalised tissue) from the field. Although this sounds for like a scrub, wash and little tiding up, it is far more complex than that. The surgeon should ideally try to re create the entire surgical field that could be potentially be contaminated. This is perhaps the most difficult task as it involves navigating through inflamed secondary surgical planes. A strong lookout for the foci in most cases around implants or fracture site is where one FINDS GOLD!.
A thorough and if possible tumor style excision then needs to be done to confidently achieve and infection free sterile surgical wound before part 2 begins. This step is called RECONSTRUCTION.
What is RECONSTRUCTION ?
This means turning an open clean wound to a closed healed wound. It is almost never simply about closing the skin directly or with tissue addition. A major challenge is – how to fill up the potential dead space that is now created – as dead space invites infection. Secondly how to shield the most vulnerable areas like implants or fracture sites with more robust , vascularized autologous tissue that can handle bacteria better. In fact, it is ideal or must for the implant(s) to be removed before closure, as this may be in the best interest of the patient.


One needs some tissue that secures the most vulnerable area in the surgical field- which is often the bone, a fracture site or the implant site. This has to be a flap that is robust , pliable and reliable – This is where plastic surgeons use own muscles as a MUSCLE FLAP.
What are muscle flaps?
Flap(s) is a plastic surgical technique to manipulate body tissues to different sites whilst keeping them alive. Muscles flaps involves manipulation of regional or remote muscles to obliterate the dead space and secure vulnerable sites with more robust and vascularized elements to help prevent deep space infections to re establish. This is the most powerful technique to combat this challenge which can potentially save limbs. The procedure requires detailed local anatomical know how and planning , coupled with vast plastic surgical experience for sound execution.
Regional or remote muscles are used to cover these vulnerable sites and fill up the dead spaces around them. It is critical that drains are left under the skin to not allow for any collection that could invite infection. Surgeons would also resort to suction assisted dressings (NPWT) and skin grafts to enable tension free closure. Perfect after care, including follow ups, antibiotics, optimization of medical problems like diabetes, smoking ,poor nutrition and proper nursing care, all contribute in going past this finish line.


Is their a time-frame for treating this problem?
Surgical site infection has a huge range, where on one end of spectrum it is a matter of few days while on the other it can go on a downward spiral with multiple failed surgical attempts and all options exhausted. Although a positive and committed approach of the patient is must, but so is understanding the gravity of the situation.
Debridement (cleaning) and reconstructive (cover) surgeries are rarely done in the same sitting and may be spaced from a few weeks to months apart and therefore the time frame of recovery entirely depends on a real time day to day update of the clinical situation rather than a surgical package.
Prominent ears
Ears are the most non geometric external feature of our face. But, nature also has methods to madness, and this is what…

Plastic surgery in management of surgical infections
What are surgical site infections? As the name suggests, it is an infection occurring at…

Breast Reduction
Breast mound not only imparts key cosmesis to the chest wall contour, but it also defines womanhood….
Open fractures of the lower limb – what makes it complex?
Introduction While fractures refer to break in the bones, one tends to ignore that a…

Facial injuries – What makes plastic surgery special?
No wonder that whenever there is an injury to the face, one tends to fear…

Hand Fractures
Injuries to the hand are common both in domestic and industrial settings. While the former…

Leave a Comment